

Dealing With Climbing’s Most Common Injuries – Part 3
With the explosive increase in the popularity of indoor bouldering, there has been a rise in lower extremity injuries, specifically knee injuries. In this third article outlining common climbing injuries (here are the links to part one and part two), we examine meniscal tears, an increasingly common knee injury in climbing.
-

Dealing With Climbing’s Most Common Injuries – Part 3

What is affected?
- A meniscus is a fibrous cartilage padding within a joint that acts as a cushion.
- There are two menisci in the knee, the medial (inner) meniscus and lateral (outer) meniscus.
-
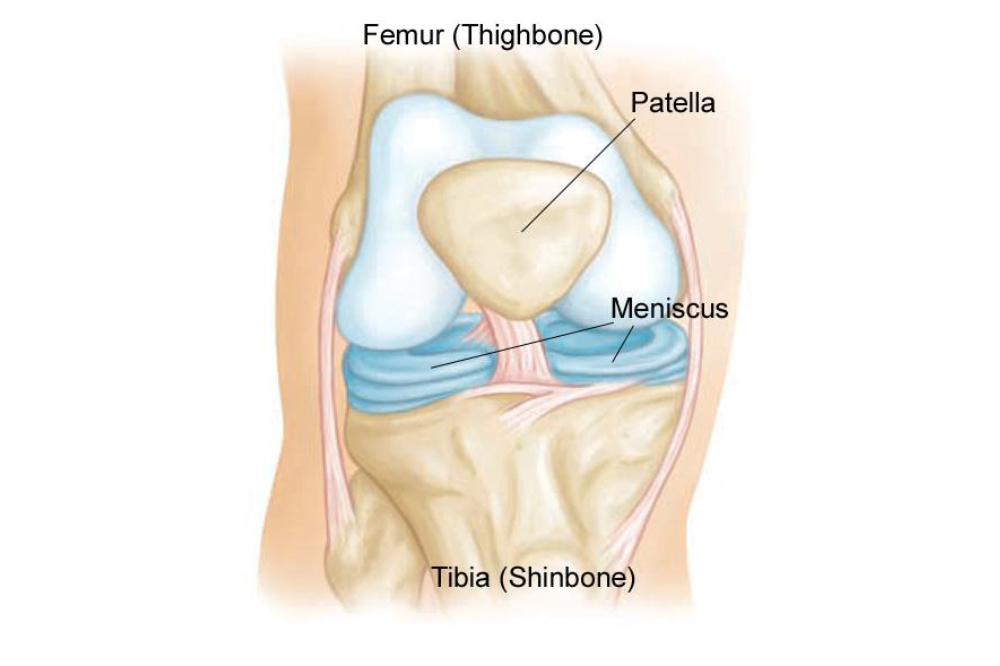
Image from: https://orthoinfo.aaos.org/en/diseases--conditions/meniscus-tears/

How does this injury happen?
A meniscal tear results from a grinding and twisting motion. In climbing, the at-risk movements include (1):
- High knee (A)
- Drop knee (B)
- Heel hooks (C)
- Falls (D)
-
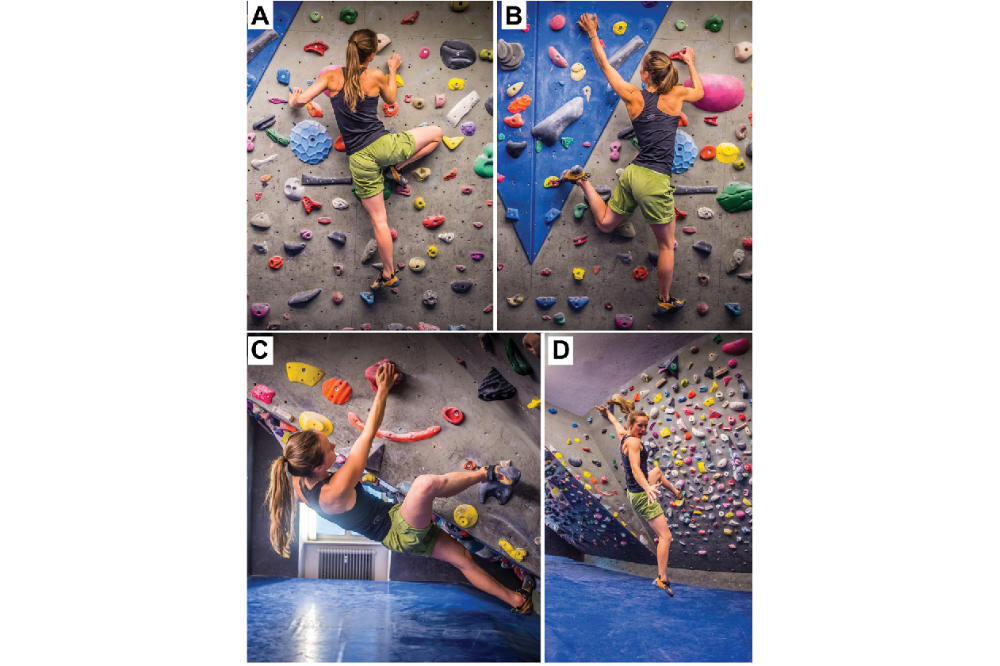
Image from: Mechanisms of Acute Knee Injuries in Bouldering and Rock Climbing Athletes. The American Journal of Sports Medicine (2020).

What are the symptoms?
- Climbers may feel a popping sensation at the time of injury
- There is typically same-day swelling and pain.
- There may be pain with twisting through the knee.
- The sensation of the knee giving way is also common.
- Climbers may have difficulty straightening the knee.
- Many injured climbers also experience locking or catching in the knee.
Load the knee slowly and train specifically for positions such as drop knees – don't just use them on the fly!
How is it diagnosed?
- An assessment of the mechanism of injury, a climber's physical history and a clinical examination are the first steps towards diagnosing the injury.
- X-rays may be used to rule out damage to the bone.
- Ultrasounds are typically not very helpful in examining menisci.
- MRIs are usually only ordered if surgery is being considered or there is an unclear diagnosis.
How is it treated?
- As with many injuries, rest, ice, anti-inflammatories are the first line of treatment.
- Surgery in the adult population is only required for certain types of tears and unstable tears. (2) Success after surgery varies depending on the type of tear, the patient's age, and overall health.
- Hyaluronic acid has not been studied in-depth for acute meniscal tears. Small studies have demonstrated mixed results for chronic degenerative tears. (3,4)
- There is not enough data to support platelet-rich plasma injections with or without surgery. (5) Other biological agents, such as stem cell therapy, are still being researched.
-

Adam Ondra employing an extreme knee drop.

How can I prevent epicondylitis?
- Climbers should strengthen the muscles around the knee and also around the hip.
- Load the knee slowly and train specifically for positions such as drop knees – don't just use them on the fly!
- Wear proper footwear that provides sufficient control and grip to minimize slipping and unexpected loading.
- Avoid training when injured or tired.
References:
- Lutter, et al. Mechanisms of Acute Knee Injuries in Bouldering and Rock Climbing Athletes. The American Journal of Sports Medicine, 2020. doi:10.1177/036354651989993
- Laible C, Stein DA, Kiridly DN. Meniscal repair. J Am Acad Orthop Surg. 2013;21(4):204–213.
- Başar, Betül et al. 'Comparison of Physical Therapy and Arthroscopic Partial Meniscectomy Treatments in Degenerative Meniscus Tears and the Effect of Combined Hyaluronic Acid Injection with These Treatments: A Randomized Clinical Trial'. 1 Jan. 2021 : 1 – 8.
- Babwah T, Pattron R & Adolph, C. Intra Articular Hyaluronic Acid (Hylan G-F 20) in patients with knee meniscal injuries: A retrospective cohort study. Annals of Musculoskeletal Medicine, 2017. 1:39-42. 10.17352/amm.000008.
- Haunschild ED, Huddleston HP, Chahla J, Gilat R, Cole BJ, Yanke AB. Platelet-Rich Plasma Augmentation in Meniscal Repair Surgery: A Systematic Review of Comparative Studies. Arthroscopy: The Journal of Arthroscopic & Related Surgery, 2020; 36(6): 1765-1774
Join the discussion of this and other climbing related stories at www.ontarioclimbing.com/forum/

Dr. Liang is involved in medical education, leadership roles, patient education and research, and has interests in exercise as medicine, sports nutrition and performance arts medicine. She has worked with various Varsity Blues teams as well as the National Ballet of Canada, the 2015 Pan Am Games, the Mississauga Steelheads, the Around the Bay Road Race and the Toronto Rock Lacrosse team. She is currently the Company Physician for Canada's Ballet Jörgen.
Dr. Liang lives with her husband and two sons in Burlington. In her spare time, she loves being active (doing hot yoga, step aerobics, cycling and climbing), playing trumpet and piano, reading sci-fi novels, cooking and travelling. You can follow her on Instagram @drliangsportsmed.